

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
The UK Health Security Agency (UKHSA) has issued an update on the ongoing investigation into higher than usual rates of liver inflammation (hepatitis) in children across the UK.
Prof Will Irving, Professor of Virology, University of Nottingham, said:
“The occurrence of severe hepatitis in a young child is not a new phenomenon – there have been occasional cases presenting over the years, with no underlying cause identified – often referred to as non A-E hepatitis, as tests for the standard hepatitis viruses are negative. What is unusual is the increased number of such cases seen over a short space of time since January this year.
“The emergence of the UK population from a period of much less social mixing than normal has been associated with an increase in laboratory diagnoses of a whole range of virus infections, including adenoviruses, in the recent winter. If non A-E hepatitis is caused by an as yet unidentified virus, then it wouldn’t be surprising if there had also been an increase in the number of infections caused by that virus.
“There are over 80 identified adenoviruses which are known to infect humans, each given a unique number. Adenovirus 41 is a well recognised cause of a gastroenteritis illness in young children, but has not been associated with hepatitis previously. However, the increasing percentage of children fulfilling the current case definition of severe acute hepatitis in whom Ad-41 has been found cannot be ignored, and suggests that Ad-41 infection may well be linked in some way with the disease. In considering the laboratory data regarding Ad-41 infection, it is important to bear in mind that standard assays (tests) for adenovirus infection may well not be optimal for detection of this particular strain of adenovirus, and therefore samples should be sent to labs who are using the most sensitive assays for this virus.”
Prof Simon Taylor-Robinson, Hepatologist, Imperial College London, said:
“Now that the clinical details of the first few cases have been published in Eurosurveillance (https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2022.27.15.2200318), it would appear that a viral cause is likely, although this still awaits confirmation.
“Further reports have shown that 77% of UK cases have tested positive for adenoviruses (https://www.gov.uk/government/news/increase-in-hepatitis-liver-inflammation-cases-in-children-under-investigation), although it should be remembered that exposure to a virus does not necessarily imply causality.
“Adenoviruses are viruses that can normally cause the common cold in adults, but also diarrhoea, abdominal pain and vomiting in children. Sometimes symptoms can be more severe and can rarely cause liver inflammation. It is not uncommon to have adenoviruses in spring time. Given their seasonality, it may be that the past two years has seen children isolated away from their peers and thus not contracting the usual childhood viral illnesses that build up immunity. Thus, contact now to viruses like adenoviruses may account for the more exaggerated symptoms of some of these previously isolating children.
“And there are other viruses around too – COVID-19 has been associated with inflammation of many other body organs. At the moment we don’t know for certain what the cause is but the authorities are investigating intensively. It is also difficult to work out cause and effect because viruses can be common anyway, so might be present but not necessarily the cause.
“Treatment is usually supportive – with hydration and management of temperature – because the problem normally resolves. The liver has an amazing ability to regenerate itself after an insult – generally within a few days or weeks things settle back down with this supportive treatment. If blood tests are significantly abnormal treatment would be in a specialised hospital as in rare cases, the liver injury can require more specialised medical intervention.
“Now that medical authorities are alerted to the situation, it will ensure that any child displaying symptoms should get earlier and more effective care. If parents are worried about symptoms in their children they should contact their doctor.
“If adenoviruses are shown to be the underlying cause, it means the same sorts of precautions as for other viruses with attention to hand washing and alcohol sanitisers, for example, to prevent viral spreading. This is something with which the public is familiar these days due to COVID.”
Prof Deirdre Kelly, Professor of Paediatric Hepatology at the University of Birmingham; and Liver Unit at the Birmingham Women’s & Children’s Hospital, said:
“It’s important to emphasise that this is unusual but is still a rare occurrence in this age group of children. Nearly all recover spontaneously. A small percentage have needed liver transplants (<10%).
What is hepatitis and is it common in children?
“Hepatitis means an inflammation of the liver. It is a common reaction of the liver to many viruses, certain drugs and poisons and auto immune or genetic diseases.
Does hepatitis always have a cause?
“In about 80% of cases it has a cause, but we also see severe inflammation for which we do not find a cause: this is non-A-E Hepatitis.
How is sudden onset hepatitis (liver inflammation) usually treated?
“It depends on the cause. Antiviral drugs if relevant or treatment for autoimmune disease.
What sorts of investigations will be going on to determine why these cases might have happened?
“Test of liver function, liver damage, look for relevant viruses: hepatitis A, B, C, E; CMV, EBV, parvo, adeno; and auto immune markers, DNA.
Would we expect the number of reported cases to rise once an issue has been raised and clinicians have been asked to be alert to possible cases?
“Yes as milder cases might not be reported otherwise.
What do we know about adenoviruses?
“They normally cause mild respiratory illnesses. They rarely cause liver inflammation unless immunosuppressed.”
Prof Anil Dhawan, Professor of Paediatric Hepatology and Head of the Hepatocyte Biology and Transplantation Group at King’s College London; and Director of the Paediatric Liver GI and Nutrition Center and MowatLabs, and Director of Research and Innovation at King’s College Hospital, said:
What is hepatitis and is it common in children?
“Hepatitis is inflammation or swelling of liver. Hepatitis is uncommon in children. We suspect hepatitis when we see abnormal liver enzymes that reflect damage to liver cells. To see inflammation we have to do a liver biopsy, which is an invasive test and not done for every hepatitis case.
Does hepatitis always have a cause?
“Causes of hepatitis in children include viral infections, autoimmune (immune injury against self), drugs or toxins, inherited genetic defects. But despite extensive investigations sometimes it is not possible to identify a causative agent or factor. Causes also depend on the age of the child, like in infants perinatal infections while in adolescents infections like glandular fever or autoimmune hepatitis are among the common causes. Hepatitis A is very common cause in Asian, African and South American countries but not in UK.
How is sudden onset hepatitis (liver inflammation) usually treated?
“This depends on the cause and severity. Antiviral agents can be used when there is a treatable viral cause like Herpes virus, or other viruses like Hepatitis B or C, or Adenovirus. If the liver involvement is severe, reflected in abnormal clotting tests (we call this synthetic failure leading to acute liver failure), a patient may need urgent liver transplantation. In children where there is no identifiable and treatable cause, close monitoring with general support (fluids, nutrition) is practised. Children usually will require hospitalisation and input from a liver centre in their care. Excessive use of paracetamol beyond recommended limits can cause liver dysfunction with high liver enzymes, and sometimes liver failure.
What sorts of investigations will be going on to determine why these cases might have happened?
“Public Health England and other organisation are working with clinicians (liver experts and others) to investigate all possible causes like viral or toxins. Currently in the hospitals when we are managing these children we are excluding the conditions that we usually see (that are known viruses, autoimmune conditions); in addition we are carrying out special tests to identify any new viruses under the guidance of virologists and PHE.
Would we expect the number of reported cases to rise once an issue has been raised and clinicians have been asked to be alert to possible cases?
“That is partly correct but numbers are much higher that we saw in pre pandemic years.”
Dr Zania Stamataki, Associate Professor in Viral Immunology, Centre for Liver and Gastrointestinal Research, University of Birmingham, said:
“Adenoviruses are a family of common viruses that can cause flu-like and gastrointestinal disease that usually resolves without causing lasting damage. Particularly in children, adenoviruses cause mild symptoms. Liver inflammation (known as hepatitis) caused by adenovirus is uncommon in the young, with the exception of immunocompromised children.
“The liver is the largest internal organ with the remarkable ability to regenerate. Even if over half of our liver is removed, it can grow back to the size needed to support the body, and this is why we can donate part of our liver to patient with liver failure. If a virus, fatty diet, drug or toxin damages the liver, it needs to cause catastrophic injury to lead to liver failure requiring a transplant. Understanding the cause of liver injury is critical for early intervention, to give the liver a chance to repair itself.
“If viral disease is suspected as the cause of liver injury, we need to establish if it is the virus or the immune system that is rapidly damaging the liver. This way we can decide whether to treat with antivirals or anti-inflammatory medicines. Most of the children with hepatitis have tested positive for adenovirus infection which is circulating now, however the liver inflammation may have been caused by a previous infection that has now cleared. Sudden onset hepatitis may also be caused by a combination of insults to the liver, including viruses, toxins or drug treatments.
“The rising incidence of children with sudden onset hepatitis is unusual and worrying. If an adenovirus is to blame, this could be a new variant of adenovirus that may cause liver injury in children with naïve/immature immune systems. But we need to know more to be sure. Alternatively, if adenovirus is the culprit for hepatitis in children that are otherwise well, we ought to look for other infections and environmental causes that could exacerbate adenoviral inflammation.”
Prof Sheila Bird, Formerly Programme Leader, MRC Biostatistics Unit, University of Cambridge, said:
“Today’s update from UKHSA is economical with its statistics.
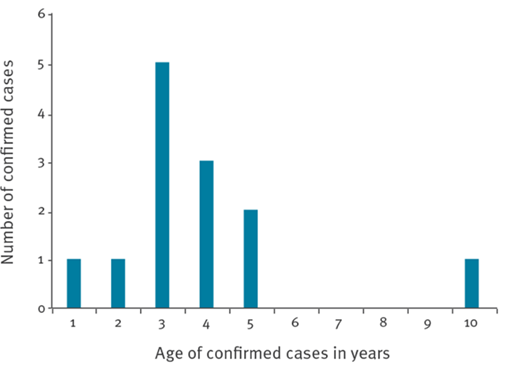
“Unlike the report last week on Scotland’s then 13 cases (now 14), see Figure, UKHSA does not report on the age-distribution of the UK’s 108 cases: England 74; Scotland 14; Wales and Northern Ireland 15. The age-distribution of Scotland’s cases, predominantly between 3 and 5 years, and their concentration in time contributed to the alert that was promptly raised by the Glasgow Hospital for Sick Children1.
“Hence, in addition to reporting cases by the date of their hospitalization, UKHSA should surely report the children’s age-distribution. Is the UK-wide distribution as concentrated as Scotland’s?
“Eight of the 108 children have received a liver transplant, presumably as super-urgent cases. Over the past 5 years (April 2016 to March 2021), UK has performed 350 deceased-donor paediatric liver transplants (i.e. recipient aged 16 or younger; about half aged 1-10 years); 56/350 (16%, 95% CI: 12% to 20%) have been super-urgent: about 11 super-urgent paediatric liver transplants per annum from deceased donors2. Eight in the first 104 days of 2022 (under 30% of the year) are thus notable.
“UKHSA is economical in its reporting on the presence of adenoviruses: present in “77% of cases tested”. Key omission is how many of the 108 cases had been “tested”. For example, 11 were tested of Scotland’s original 13 cases with 5/11 positive for adenovirus1. For transparency and to enable evidence synthesis, please qualify percentages by numerator/denominator.
“Last week, I commented that reporting delay needed to be ruled out as an explanation for then 49 out of 10.21 million children aged under 15 years [4.8 per million] in England versus 25 out of 1.76 million in the rest of UK [14 per million].
“UKHSA has not addressed reporting delays. Currently, England has 79 cases under investigation [7.7 per million children under 15 years] versus 29 in the rest of the UK [16 per million children under 15 years]. But, a commonly reported case-rate across UK would yield expected case-counts of 92.1 for England and 15.9 in the rest of the UK, from which the observed counts differ significantly (p < 0.01). Is this difference of material importance or a reflection on reporting delays in England?”
1 https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2022.27.15.2200318
Comments sent out 13/04/2022 on hepatitis in children: https://www.sciencemediacentre.org/expert-reaction-to-ukhsa-investigating-74-cases-of-hepatitis-in-children/
Declared interests
None received.