

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
A study published in PLOS ONE looks at body mass index (BMI) and all-cause mortality in a U.S. population.
Dr George Savva, Statistician, Quadram Institute Bioscience, said:
“This large study and carefully conducted study of a representative group of US adults reveals a complex relationship between weight, health and mortality as we age. Death rates for different groups of people (defined by age, sex and ethnicity) were compared over up to 20 years. Two different data sources were used and both present a similar picture.
“A wide range of potentially confounding variables were included and the authors were careful not to adjust for potentially mediating factors such as diabetes. The only potential concern there is that while the authors describe adjusting for age they did not describe how this was done. Since age is the most important determinant of mortality risk it is possible there is some residual confounding there but it’s not easy to say in which direction this might affect the results.
“Overall the results reveal a typical U-shaped relationship between weight and mortality, with those at the extremes of high and low BMI having the highest death rates in many groups, and a smaller effect for those closer to a ‘healthy’ weight. The paper shows no associations with mortality for those who might be considered slightly overweight (BMI between 25 and 27.5) compared to those at a ‘healthy’ weight (BMI 20-24.9).
“The press release downplays the increase in mortality seen in other groups that would be considered overweight or obese (those with a BMI over 27.5), and a cursory reading might give the impression that weight is not relevant to mortality risk. The headline of the press release is irresponsible in my view, since people may not distinguish between overweight and obesity, and may conclude that the paper shows all weight gain is benign. If fact the paper consistently shows an increased risk of death associated with obesity (BMI>30).
“It’s important to remember that a BMI of 30 or more still includes around a third of the US population and more than 1 in 4 UK adults, and so even if the excess risk is restricted to this group as the paper suggests, it still potentially affects a very large number of people, particularly in middle age.
“For otherwise healthy people under 65, being overweight (BMI between 27.5 and 29.9) was associated with an approximately 20% increase in mortality rate. For unhealthy people or smokers the association is lower and is only seen at a BMI of 30 or higher, presumably because other causes of death that are not weight-related are more common.
“As we expect, for people aged 65 and older the risk of death is not as closely linked to weight, with an increase in mortality typically seen only at a BMI of 30 or 35 depending on other factors. We know for older people that weight loss in the form of low muscle mass is an aspect of frailty or other chronic diseases, and this study is unable to disaggregate this issue. The paper also cannot directly attribute weight as the cause of any differences in death rate.”
Dr Adam Jacobs, Senior Director, Biostatistical Science, Premier Research, said:
“The paper did not find that BMI does not increase mortality. At the highest ranges of BMI, there was a clear link between BMI and mortality. What it did find was that being overweight, but not obese, (ie BMI in the range 25-30) was not associated with increased mortality. This has been found in other studies also, and may well be true. However, even in this study, there was a clear increase in mortality risk associated with obesity.
“What they claim to have found was that in older adults (> 65 years) there was no association between BMI and mortality even into the lower end obese range (30-35 kg/m2). There are a couple of reasons to treat this finding cautiously. First, it’s a subgroup. Subgroup analyses always need to be treated with caution, as the more subgroups you examine, the greater the chance of spurious findings. And second, it’s possible that there is some kind of healthy survivor bias in the older age group. In other words, older patients whose obesity puts them at particularly increased mortality risk are probably not in the study as they would already be dead before they reach that age.”
Prof Tom Sanders, Professor emeritus of Nutrition and Dietetics, King’s College London, said:
“The findings of this new study are consistent with data from the prospective studies collaboration (Lancet 2009, 373: 1083-1096) in 900,000 adults which also showed that overweight in older adults is not associated with increased mortality especially in females. The effects of BMI 30-35 in this new study were associated with increased mortality in young but not in older participants. It also confirms that being underweight BMI <20 is associated with increased mortality. Cigarette smoking in contrast has a huge effect on all cause mortality and smokers tend to be lighter in weight than non-smokers, so this can cause problems when interpreting studies such as these.
“The prospective studies show those that overweight/obese smokers have a greatly enhanced risk of cardiovascular disease compared to comparisons of those non-smokers of the same weight. It is this combination that appears to be particularly deadly especially in women. Non-smokers who are overweight/obese (BMI less than 35) have a lower risk of premature mortality than normal weight smokers. This present study focuses on the risks of overweight/obesity in non-smokers and broadly confirms this. However, 42 percent of the sample were smokers/past smokers.
“A further limitation is that adjustment for co-morbidities, some of which are obesity related and cardiovascular disease such as metabolic syndrome, were made which would dilute effects of obesity. What is particularly worrying about this new US data is how severe obesity (BMI > 40) has increased in women, especially those of Hispanic and Black ethnicity.
“Morbidity is probably a more important measure of health than all cause mortality. The main hazard of overweight (BMI 25 – 29.9) and moderate obesity (BMI 30-35) is a three times greater risk of developing diabetes which contributes to cardiovascular disease, renal failure and blindness. The risks of diabetes are also greater for people of South Asian origin with increasing BMI compared to people of European descent.”
Prof Naveed Sattar, Professor of Metabolic Medicine, University of Glasgow, said:
“This paper does not add anything new. We know that BMI often displays a U shaped curve with mortality but this is due to many people (particularly older) at lower end of the BMI range having unintentional weight loss due to illness.
“Looking at the BMI to mortality pattern in younger non-smokers without any evidence of illness at baseline is best one can do to get closer to the truth about BMI and its association with mortality. The authors have tried to do this but only included under 65 group but they could have looked at even younger groups. Even so, here the data show a more linear pattern with higher BMIs associated with greater mortality.
“It is important to add, however, that the BMI to mortality link is perhaps no longer the important metric as many chronic illness can now be better treated and large reductions in cardiovascular and cancer mortality have also occurred due to better prevention or care. What matters more now is how excess weight influences the risk of developing one or more conditions, so called multimorbidity, and here the data from research as a whole are clear. We know from other evidence that the higher our weight, the greater the risks of developing multiple conditions such as diabetes, arthritis, fatty liver, hypertension, heart failure, kidney disease, gout, multiple cancers, heart disease and the list goes on and on. These conditions in turn adversely influence peoples quality of life and their happiness. It is these ‘quality of life’ metrics we need to focus more on, and, if possible, try to improve with relevant interventions at multiple stages of life and via environmental changes.”
Dr Katarina Kos, Senior Lecturer in Diabetes and Obesity, University of Exeter, said:
“The report of a somewhat lower risk of dying in the overweight BMI range is surprising and strongly contrasted with the 21–108% increased risk of mortality for men and women with a BMI above 30 kg/m2.
“We should remember that this is a US study and data is based on the US body shape; that the weight data and reported illness were obtained from individual’s self-reports; and no true adjustments can be made to smoking or more precisely to nicotine use with vaping. These shortcomings will to some extent be reflected in the data and make interpretation difficult. It is not possible to extrapolate how applicable the observed trend is to the British population.
“Being overweight is the norm with more than 70% of the adult population in the UK aged above 45 being overweight or obese, of which more than 30% are obese. With a steady increase in future population’s BMI and our own weight as we become older, this does by no means mean that we can relax in our efforts in weight management.”
Dr Adam Collins, Associate Professor of Nutrition, University of Surrey, said:
“Given the large cohort size in this observational analysis, I read the paper by Visaria and Setoguchi with interest. The authors acknowledged some of the limitations in the data analysis. Still, this paper serves as further convincing evidence to question the validity of BMI as a marker of health.
“BMI only reflects body weight adjusting for height, as a proxy for “excess” weight. From a health perspective, it is assumed that excess weight directly reflects excess body fat, as excess adiposity (body fatness) is associated with increased health risk. The observation that within the BMI range of 22.5 to 30 kg/m2, no change in mortality is likely a consequence of the relatively weak association between BMI and adiposity within this BMI range. As the authors acknowledged, differences in lean mass between individuals are a potential critical confounder without measures of body composition.
“Beyond overall adiposity, how the fat is distributed will significantly influence health outcomes, specifically central adiposity (fat around the waist). The authors acknowledged that including waist circumference would have been helpful as a crude marker of central adiposity. However, this may not truly reflect the variation in fat distribution seen in people within a BMI range of 22.5-30. It is the fat on the “inside” that is most impactful. Specifically, intrabdominal (e.g. visceral) and ectopic fat (fat where it shouldn’t be, e.g. inside of muscle and organs). Indeed, individuals of the same BMI and waist circumference can have markedly different levels of intraabdominal or ectopic fat. This partly describes how some individuals can be metabolically obese, despite having a normal or overweight BMI. In a lean population, this TOFI phenotype (thin on the outside, fat on the inside) has been identified (from MRI data) as a hidden health risk. In contrast, for some being overweight or obese can be relatively “benign” as they are metabolically healthy, possibly due to how they store that fat but also other diet and lifestyle factors (hence the term “fat but fit”). Weight history is another influencing factor alluded to by the authors. Weight loss of 5-10% will significantly impact health risks. Some Individuals who are overweight were likely recently obese. Especially given that 1 in 4 adults in the UK (including 1 in 3 women) are trying to lose weight most of the time.
“The last point to make, which is overlooked somewhat in this paper, is the U-shaped curve when looking at the BMI plotted against mortality. In other words, having a low BMI is also of increased risk. This rise in mortality risk is noticeable below a BMI of 20, perhaps in younger individuals but is elevated at BMIs below 22 in the older group. This suggests that potential loss of lean body mass and musculoskeletal health may contribute to risk, including the influence of sarcopenia in older adults.”
Dr Baptiste Leurent, Lecturer in Medical Statistics, University College London, said:
“This paper reports the results of a recent retrospective cohort of over 500,000 adults in the US looking at the association between BMI and mortality.
“The press release could suggest no association between BMI and mortality was found. However, this would be misleading.
“The association between BMI and mortality is well represented in Figure 1 (copied below). It represents the risk of mortality, compared to a reference group (BMI=22.5 to 25 kg/m2). We can see that, although there is not much difference in mortality among the 18.5-30 groups (normal and overweight), there is a clearly higher mortality in the underweight (<18.5) or obese (>30) groups.
“This paper found an unequivocal association between BMI and mortality, before and after adjustment for risk factors.
“The press release title (“No increase in mortality for most overweight people”) is possibly based on the lack of significant difference between the specific “overweight” category (25-30), compared to “normal” (18.5-15) BMI category. This is interesting, and highlights that the definition of “overweight” commonly used in medical settings may not be associated with serious health conditions.
“However, the use of the word “overweight” is misleading here, as it excludes anyone with a BMI above 30. In lay language “overweight” would usually be interpreted as anyone with a weight above “normal” and would include obese patients.
“Overall, although there was not apparent higher mortality in the “overweight” group, patients with higher BMI (>30 kg/m2) had a clear higher mortality risk, somewhere between 20% to 100% higher than those with a “normal” BMI.
“This study adds to the literature on the association between weight and health risk, based on a recent and large dataset. But it does not provide much novel information, except indicating a limited increase in mortality risk in the “overweight” category.”
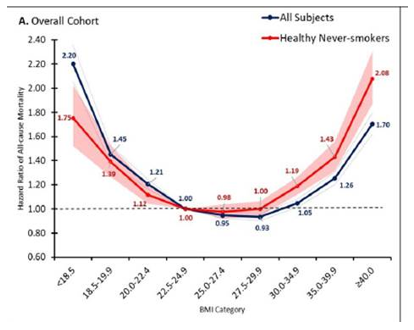
Figure 1 from: Visaria A, Setoguchi S (2023) Body mass index and all-cause mortality in a 21st century U.S. population: A National Health Interview Survey analysis. PLoS ONE 18(7): e0287218. https://doi.org/10.1371/journal.pone.0287218
‘Body mass index and all-cause mortality in a 21st century U.S. population: A National Health Interview Survey analysis’ by Aayush Visaria and Soko Setoguchi was published in PLOS ONE at 19:00 UK time on Wednesday 5 July 2023.
DOI: 10.1371/journal.pone.0287218
Declared interests
A study published in PLOS ONE looks at body mass index (BMI) and all-cause mortality in a U.S. population.
Dr George Savva, Statistician, Quadram Institute Bioscience, said:
“This large study and carefully conducted study of a representative group of US adults reveals a complex relationship between weight, health and mortality as we age. Death rates for different groups of people (defined by age, sex and ethnicity) were compared over up to 20 years. Two different data sources were used and both present a similar picture.
“A wide range of potentially confounding variables were included and the authors were careful not to adjust for potentially mediating factors such as diabetes. The only potential concern there is that while the authors describe adjusting for age they did not describe how this was done. Since age is the most important determinant of mortality risk it is possible there is some residual confounding there but it’s not easy to say in which direction this might affect the results.
“Overall the results reveal a typical U-shaped relationship between weight and mortality, with those at the extremes of high and low BMI having the highest death rates in many groups, and a smaller effect for those closer to a ‘healthy’ weight. The paper shows no associations with mortality for those who might be considered slightly overweight (BMI between 25 and 27.5) compared to those at a ‘healthy’ weight (BMI 20-24.9).
“The press release downplays the increase in mortality seen in other groups that would be considered overweight or obese (those with a BMI over 27.5), and a cursory reading might give the impression that weight is not relevant to mortality risk. The headline of the press release is irresponsible in my view, since people may not distinguish between overweight and obesity, and may conclude that the paper shows all weight gain is benign. If fact the paper consistently shows an increased risk of death associated with obesity (BMI>30).
“It’s important to remember that a BMI of 30 or more still includes around a third of the US population and more than 1 in 4 UK adults, and so even if the excess risk is restricted to this group as the paper suggests, it still potentially affects a very large number of people, particularly in middle age.
“For otherwise healthy people under 65, being overweight (BMI between 27.5 and 29.9) was associated with an approximately 20% increase in mortality rate. For unhealthy people or smokers the association is lower and is only seen at a BMI of 30 or higher, presumably because other causes of death that are not weight-related are more common.
“As we expect, for people aged 65 and older the risk of death is not as closely linked to weight, with an increase in mortality typically seen only at a BMI of 30 or 35 depending on other factors. We know for older people that weight loss in the form of low muscle mass is an aspect of frailty or other chronic diseases, and this study is unable to disaggregate this issue. The paper also cannot directly attribute weight as the cause of any differences in death rate.”
Dr Adam Jacobs, Senior Director, Biostatistical Science, Premier Research, said:
“The paper did not find that BMI does not increase mortality. At the highest ranges of BMI, there was a clear link between BMI and mortality. What it did find was that being overweight, but not obese, (ie BMI in the range 25-30) was not associated with increased mortality. This has been found in other studies also, and may well be true. However, even in this study, there was a clear increase in mortality risk associated with obesity.
“What they claim to have found was that in older adults (> 65 years) there was no association between BMI and mortality even into the lower end obese range (30-35 kg/m2). There are a couple of reasons to treat this finding cautiously. First, it’s a subgroup. Subgroup analyses always need to be treated with caution, as the more subgroups you examine, the greater the chance of spurious findings. And second, it’s possible that there is some kind of healthy survivor bias in the older age group. In other words, older patients whose obesity puts them at particularly increased mortality risk are probably not in the study as they would already be dead before they reach that age.”
Prof Tom Sanders, Professor emeritus of Nutrition and Dietetics, King’s College London, said:
“The findings of this new study are consistent with data from the prospective studies collaboration (Lancet 2009, 373: 1083-1096) in 900,000 adults which also showed that overweight in older adults is not associated with increased mortality especially in females. The effects of BMI 30-35 in this new study were associated with increased mortality in young but not in older participants. It also confirms that being underweight BMI <20 is associated with increased mortality. Cigarette smoking in contrast has a huge effect on all cause mortality and smokers tend to be lighter in weight than non-smokers, so this can cause problems when interpreting studies such as these.
“The prospective studies show those that overweight/obese smokers have a greatly enhanced risk of cardiovascular disease compared to comparisons of those non-smokers of the same weight. It is this combination that appears to be particularly deadly especially in women. Non-smokers who are overweight/obese (BMI less than 35) have a lower risk of premature mortality than normal weight smokers. This present study focuses on the risks of overweight/obesity in non-smokers and broadly confirms this. However, 42 percent of the sample were smokers/past smokers.
“A further limitation is that adjustment for co-morbidities, some of which are obesity related and cardiovascular disease such as metabolic syndrome, were made which would dilute effects of obesity. What is particularly worrying about this new US data is how severe obesity (BMI > 40) has increased in women, especially those of Hispanic and Black ethnicity.
“Morbidity is probably a more important measure of health than all cause mortality. The main hazard of overweight (BMI 25 – 29.9) and moderate obesity (BMI 30-35) is a three times greater risk of developing diabetes which contributes to cardiovascular disease, renal failure and blindness. The risks of diabetes are also greater for people of South Asian origin with increasing BMI compared to people of European descent.”
Prof Naveed Sattar, Professor of Metabolic Medicine, University of Glasgow, said:
“This paper does not add anything new. We know that BMI often displays a U shaped curve with mortality but this is due to many people (particularly older) at lower end of the BMI range having unintentional weight loss due to illness.
“Looking at the BMI to mortality pattern in younger non-smokers without any evidence of illness at baseline is best one can do to get closer to the truth about BMI and its association with mortality. The authors have tried to do this but only included under 65 group but they could have looked at even younger groups. Even so, here the data show a more linear pattern with higher BMIs associated with greater mortality.
“It is important to add, however, that the BMI to mortality link is perhaps no longer the important metric as many chronic illness can now be better treated and large reductions in cardiovascular and cancer mortality have also occurred due to better prevention or care. What matters more now is how excess weight influences the risk of developing one or more conditions, so called multimorbidity, and here the data from research as a whole are clear. We know from other evidence that the higher our weight, the greater the risks of developing multiple conditions such as diabetes, arthritis, fatty liver, hypertension, heart failure, kidney disease, gout, multiple cancers, heart disease and the list goes on and on. These conditions in turn adversely influence peoples quality of life and their happiness. It is these ‘quality of life’ metrics we need to focus more on, and, if possible, try to improve with relevant interventions at multiple stages of life and via environmental changes.”
Dr Katarina Kos, Senior Lecturer in Diabetes and Obesity, University of Exeter, said:
“The report of a somewhat lower risk of dying in the overweight BMI range is surprising and strongly contrasted with the 21–108% increased risk of mortality for men and women with a BMI above 30 kg/m2.
“We should remember that this is a US study and data is based on the US body shape; that the weight data and reported illness were obtained from individual’s self-reports; and no true adjustments can be made to smoking or more precisely to nicotine use with vaping. These shortcomings will to some extent be reflected in the data and make interpretation difficult. It is not possible to extrapolate how applicable the observed trend is to the British population.
“Being overweight is the norm with more than 70% of the adult population in the UK aged above 45 being overweight or obese, of which more than 30% are obese. With a steady increase in future population’s BMI and our own weight as we become older, this does by no means mean that we can relax in our efforts in weight management.”
Dr Adam Collins, Associate Professor of Nutrition, University of Surrey, said:
“Given the large cohort size in this observational analysis, I read the paper by Visaria and Setoguchi with interest. The authors acknowledged some of the limitations in the data analysis. Still, this paper serves as further convincing evidence to question the validity of BMI as a marker of health.
“BMI only reflects body weight adjusting for height, as a proxy for “excess” weight. From a health perspective, it is assumed that excess weight directly reflects excess body fat, as excess adiposity (body fatness) is associated with increased health risk. The observation that within the BMI range of 22.5 to 30 kg/m2, no change in mortality is likely a consequence of the relatively weak association between BMI and adiposity within this BMI range. As the authors acknowledged, differences in lean mass between individuals are a potential critical confounder without measures of body composition.
“Beyond overall adiposity, how the fat is distributed will significantly influence health outcomes, specifically central adiposity (fat around the waist). The authors acknowledged that including waist circumference would have been helpful as a crude marker of central adiposity. However, this may not truly reflect the variation in fat distribution seen in people within a BMI range of 22.5-30. It is the fat on the “inside” that is most impactful. Specifically, intrabdominal (e.g. visceral) and ectopic fat (fat where it shouldn’t be, e.g. inside of muscle and organs). Indeed, individuals of the same BMI and waist circumference can have markedly different levels of intraabdominal or ectopic fat. This partly describes how some individuals can be metabolically obese, despite having a normal or overweight BMI. In a lean population, this TOFI phenotype (thin on the outside, fat on the inside) has been identified (from MRI data) as a hidden health risk. In contrast, for some being overweight or obese can be relatively “benign” as they are metabolically healthy, possibly due to how they store that fat but also other diet and lifestyle factors (hence the term “fat but fit”). Weight history is another influencing factor alluded to by the authors. Weight loss of 5-10% will significantly impact health risks. Some Individuals who are overweight were likely recently obese. Especially given that 1 in 4 adults in the UK (including 1 in 3 women) are trying to lose weight most of the time.
“The last point to make, which is overlooked somewhat in this paper, is the U-shaped curve when looking at the BMI plotted against mortality. In other words, having a low BMI is also of increased risk. This rise in mortality risk is noticeable below a BMI of 20, perhaps in younger individuals but is elevated at BMIs below 22 in the older group. This suggests that potential loss of lean body mass and musculoskeletal health may contribute to risk, including the influence of sarcopenia in older adults.”
Dr Baptiste Leurent, Lecturer in Medical Statistics, University College London, said:
“This paper reports the results of a recent retrospective cohort of over 500,000 adults in the US looking at the association between BMI and mortality.
“The press release could suggest no association between BMI and mortality was found. However, this would be misleading.
“The association between BMI and mortality is well represented in Figure 1 (copied below). It represents the risk of mortality, compared to a reference group (BMI=22.5 to 25 kg/m2). We can see that, although there is not much difference in mortality among the 18.5-30 groups (normal and overweight), there is a clearly higher mortality in the underweight (<18.5) or obese (>30) groups.
“This paper found an unequivocal association between BMI and mortality, before and after adjustment for risk factors.
“The press release title (“No increase in mortality for most overweight people”) is possibly based on the lack of significant difference between the specific “overweight” category (25-30), compared to “normal” (18.5-15) BMI category. This is interesting, and highlights that the definition of “overweight” commonly used in medical settings may not be associated with serious health conditions.
“However, the use of the word “overweight” is misleading here, as it excludes anyone with a BMI above 30. In lay language “overweight” would usually be interpreted as anyone with a weight above “normal” and would include obese patients.
“Overall, although there was not apparent higher mortality in the “overweight” group, patients with higher BMI (>30 kg/m2) had a clear higher mortality risk, somewhere between 20% to 100% higher than those with a “normal” BMI.
“This study adds to the literature on the association between weight and health risk, based on a recent and large dataset. But it does not provide much novel information, except indicating a limited increase in mortality risk in the “overweight” category.”
Figure 1 from: Visaria A, Setoguchi S (2023) Body mass index and all-cause mortality in a 21st century U.S. population: A National Health Interview Survey analysis. PLoS ONE 18(7): e0287218. https://doi.org/10.1371/journal.pone.0287218
‘Body mass index and all-cause mortality in a 21st century U.S. population: A National Health Interview Survey analysis’ by Aayush Visaria and Soko Setoguchi was published in PLOS ONE at 19:00 UK time on Wednesday 5 July 2023.
DOI: 10.1371/journal.pone.0287218
Declared interests
Dr Adam Jacobs: “No conflicts of interest to declare.”
Dr Adam Collins: “None that I can think of. The only non-Surrey activity is my role as Head of Nutrition for Form Nutrition – although this is not a direct conflict (they are a plant protein supplement company).”
Dr George Savva: “I have no conflict of interest.”
Prof Tom Sanders: “No conflicts of interest declared.”
Prof Naveed Sattar: “Have consulted for companies (Novo Nordisk, Lilly) that market weight loss drugs as well as others develop such drugs.
Have also been involved in several lifestyle trials of weight loss.”
Dr Katarina Kos: “I have no conflict of interest.”
Dr Baptiste Leurent: “No conflict of interest.”
For all other experts, no reply to our request for DOIs was received.