

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
A observational study published in the Lancet looks at impact and effectiveness of the Pfizer-BioNTech COVID-19 vaccine against infections, cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel.
Dr Gillies O’Bryan-Tear, Of the Faculty of Pharmaceutical Medicine, said:
“This real-life vaccine effectiveness study from Israel is the first such study published on a large section of a vaccinated population, owing to the rapidity of the vaccine rollout in Israel. Israel used only the Pfizer-BioNTech vaccine during the period, which they agreed to do in return for providing these population data to Pfizer when they became available. The study looked at a large number of infections – 232,268 amongst some 5.2 million people vaccinated – far more than can be analysed in a controlled trial setting. The study used public health surveillance data to ascertain the cases, so some under-ascertainment and misclassification (particularly, as the authors point out, asymptomatic infection which later became symptomatic) are inevitable. The primary analysis looked at people who had received their second dose of vaccine; national laboratory testing during the period of the study showed that the dominant variant (94.5%) was B.1.1.7 (so-called East Kent), with too few cases of the South Africa variant to analyse efficacy.
“The results show that the effectiveness of the Pfizer BioNTech vaccine was over 90% for SARS-CoV-2 asymptomatic infection, rising to over 96% for symptomatic infection, hospitalisation and death. These results mirror the clinical trial data (although the trial did not analyse asymptomatic infection) and were seen across all age groups above 16 years, and demonstrate the outstanding effectiveness of this mRNA vaccine in a real world vaccination campaign. The national incidence of SARS-CoV-2 fell rapidly during the vaccination campaign, and the authors address the question of how much of this was due to lockdown, and how much to vaccination, using incidence by age cohort to demonstrate that it was primarily the vaccine campaign which achieved this in Israel.
“Of interest to the UK, a supplementary analysis examined effectiveness of the vaccine 14-21 days after the first dose (in Israel, the second dose was given according to the clinical trial schedule, at 21 days). This showed substantial effectiveness also against hospitalisation (77%), severe or critical hospital cases (80%), and death (88%).
“This population study provides something for everyone: for those who have been critical of the UK stance of providing first doses to as many as possible and delaying the second dose, the results show that people need to receive the second dose for full effectiveness (duration of effect is not addressed in this study since follow up was insufficient). On the other hand, proponents of the delayed dosing policy can also draw comfort from the fact that even single dose effectiveness was substantial for the severe endpoints of hospitalisation and death, although less so less so for asymptomatic and symptomatic infection (49% and 63% respectively).”
Dr Peter English, Retired Consultant in Communicable Disease Control, Former Editor of Vaccines in Practice Magazine, Immediate past Chair of the BMA Public Health Medicine Committee, said:
“Israel was very quick off the mark in starting its Covid-19 vaccination, using almost exclusively the Pfizer-BioNTech vaccine tozinameran. Israel has excellent systems for collecting data on both vaccination, and disease incidence. They used a 21-day prime boost interval, so they have been quick to accumulate data on the efficacy of the two-dose response, and have been able to follow such patients up for longer than has yet been possible elsewhere.
“The authors of this paper looked at real-world vaccine effectiveness from 7 days after the second dose of vaccine. This 7-day post second dose interval is appropriate.
“It takes the immune system some time to respond to the first exposure of dose of vaccine – immunity to Covid-19 vaccines seems to continue to improve for at least five weeks after the first dose.
“Once the immune system has been effectively “primed” by the first exposure, however – and this requires an adequate prime-boost interval – then, following a subsequent exposure (e.g. a dose of vaccine), there is a very rapid increase in antibody levels, and a rapid mobilisation of the cellular immune responses. This happens within a few days, so an interval of 1 week after the second dose is reasonable; one would expect the immune response to have maximised by then.
“I would expect a longer prime-boost interval to further enhance the eventual effectiveness of the vaccine.
“This is an observational study, rather than an experiment. The authors compared the rates of Covid-19 disease (of varying severity) in people who had received their second dose of vaccine at least 7 days previously, with rates in people who were unvaccinated. They write: “During the analysis period (Jan 24 to April 3, 2021), there were 232 268 SARS-CoV-2 infections, 7694 COVID-19 hospitalisations, 4481 severe or critical COVID-19 hospitalisations, and 1113 COVID-19 deaths in people aged 16 years or older.”
“These are large numbers allowing a fair amount of precision in the estimates of disease rates.
“Converting the results section of the abstract to a (more easily understandable, to me at least) table, they found:
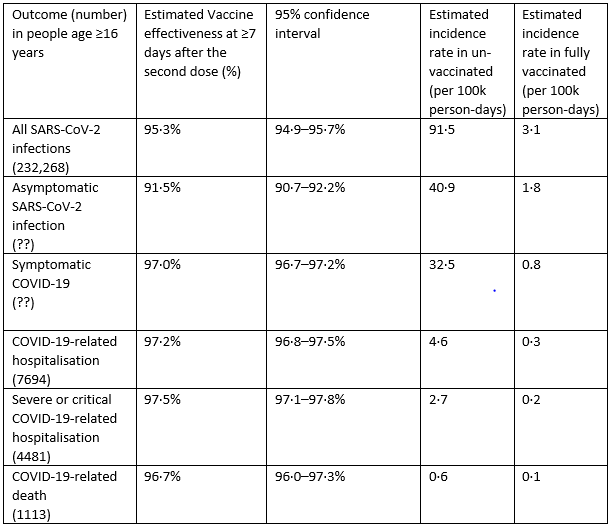
“As we would expect from previous studies, the vaccine is most effective at preventing critical illness and death, and progressively less effective at preventing less severe outcomes. Nevertheless, it appeared to be over 90% effective at preventing asymptomatic infection. Taken together with data from other studies showing that people who became infected despite having had at least one dose of vaccine were less likely to be infectious, this is extremely reassuring: it means that vaccination does have the potential to induce herd immunity. (This does require a sufficient proportion of the population to have been vaccinated or have become immune from infection; and the proportion who need to be immune relates to the infectious of the virus. This is what R0 represents. Some of the newer variants, such as the B.1.1.7 variant, are more infectious with a higher value of R0 than the original virus, increasing the proportion of the population who need to be immune before herd immunity is achieved.)
“This is reflected by the “marked and sustained declines in SARS-CoV-2 incidence corresponding to increasing vaccine coverage” – including in unvaccinated people.
“The effectiveness was in all ages – Table 2 shows this clearly, with no significant difference in effectiveness for any of the outcomes between age groups (the confidence intervals overlap). This study thus provides further evidence of effectiveness, despite immunosenescence, even in the oldest age-group (≥85 years).
“The study period was one in which the B.1.1.7 variant was circulating widely, so this study demonstrates the vaccine’s effectiveness against this variant, as well as against the original variant. The number of cases of the B.1.351 variant, first identified in South Africa, was too small to estimate vaccine effectiveness against this variant.
Answers to questions:
Does the press release accurately reflect the science?
“Yes.
Is this good quality research? Are the conclusions backed up by solid data?
“Yes, this was an observational study. Israel has excellent systems for data collection, and the large numbers of outcomes provide very robust data.
Have the authors accounted for confounders? Are there important limitations to be aware of?
“The authors address these clearly in their discussion; in short, while cofounders are not completely eliminated, the quality of Israel’s data collection systems and the large numbers mean that they are unlikely to have contributed significantly to the results, and the results are thus robust.
Is there any overspeculation?
“No.”
Prof Jonathan Ball, Professor of Molecular Virology, University of Nottingham, said:
“These data confirm the Pfizer mRNA vaccine provides very high protection from serious COVID19 disease and death – even in older more vulnerable people. Importantly, the study shows that two doses of the vaccine significantly increase levels of immunity and protection. This is why it is important that people get both doses, and if UK vaccine policy changes to get a third dose if offered in the autumn.
“Topping up your immunity with the vaccine boost will be even more important with the emergence of new variants that might have acquired genetic changes that make them more resistant to the immunity generated by vaccines or following natural infection. Therefore, it will be important to continue to monitor the potential impact of virus change and vaccine effectiveness.”
‘Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data’ by Eric J Haas et al. was published in the Lancet at 23:30 UK time on Wednesday 5 May 2021.
DOI: 10.1016/S0140-6736(21)00947-8
Declared interests
Dr Gillies O’Bryan-Tear: “Former Head of Vaccine Clinical Development, GSK. I am a pharmaceutical physician, semi-retired and have worked in a variety of fields, including oncology (cancer) drug development and vaccines development. Dr O’Bryan-Tear is Chief Medical Officer of Scancell plc, an early stage listed company developing vaccines for Covid-19.”
Dr Peter English: “No conflicts of interest to declare.”
Prof Jonathan Ball: “Receiving UKRI funding to develop DNA-based next-generation COVID19 vaccines.”