

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
A study published in The Lancet Infectious Diseases looks at household transmission and viral load kinetics of the SARS-CoV-2 delta variant in vaccinated and unvaccinated individuals in the UK.
This Roundup accompanied an SMC Briefing.
Prof Sheila Bird, Formerly Programme Leader, MRC Biostatistics Unit, University of Cambridge, said:
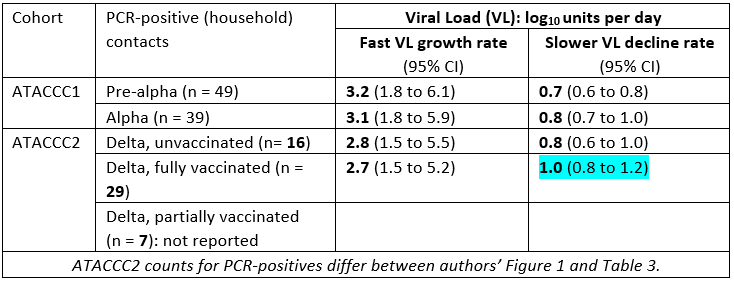
“Eligible recruits for ATACCC2 were contacts notified within 5 days of index-case symptom onset: hence most were members of the household of the index case. Within households, index case was defined as the first household-member to have a PCR-positive swab but another member might already have been infected. Unlike the ATACCC1 study (September 2020 to March 2021), the ATACCC2 study (25 May to 15 September 2021) was relaunched specifically to investigate delta variant cases in Bolton as well as in Greater London with early recruitment focused on West London where, as in Bolton, incidence was highest. Hence, some caution is warranted as any between-study whether geographical or other recruitment changes, may confound the comparison between delta and earlier variants.
“Participation-rates for ATACCC’s requested 20-day sampling of contacts’ upper respiratory tract are not reported. ATACCC2’s 163 index cases gave rise to 232 non-index contacts, 206 of whom were household contacts: 53/206 (26%) were PCR-positive household contacts. None of the 26 participating non-household contacts was PCR-positive. The 53 PCR-positive household contacts were 31/126 (25%) fully vaccinated household contacts vs 15/40 unvaccinated household contacts and 7/39 partially vaccinated (7+ days from single vaccination to exposure). Low denominators make inference foolhardy.
“Similarly, viral load growth rates (to peak) and rates of decline (from peak), when spurious accuracy is not a distraction, leave readers saddened that such a valuable study could not have been resourced to recruit nine times as many household-contact-participants and hence reduce the width of growth rate confidence intervals by a factor of 3. Faster fully vaccinated delta-decline rate is perhaps a hopeful signal. If study recruitment matched analytical power, we learn faster and more.
“An intriguing finding, that peak viral load increases with age, should be picked up by NHS Test and Trace. Large-scale investigation of ln ct-value (as proxy for viral load) for household vs external close contacts be can designed which are constrained by interval between exposure to index case and PCR-positive swab-date (to capture near-peak) and control for age, gender and vaccination status of both putative index case and PCR-positive contact. Large-scale investigation – lacking serial PCRs – will be much noisier that ATACCC’s bespoke design, which is why ATACCC merits greater support from the funder and public alike.”
Prof Keith Neal, Emeritus Professor of the Epidemiology of Infectious Diseases, University of Nottingham, said:
“This paper contributes to:
• Understanding why Delta is now the predominant variant worldwide. Delta is able to spread between vaccinated people in a way previous variants did not. Virus levels are similar between vaccinated and unvaccinated individuals but fall faster in vaccinated people.
• There is evidence of waning with a greater risk of infection the longer after the second dose of vaccine.
• Vaccinated household contacts have a significant risk of infection and NO requirement to isolate if a household contact should be urgently reconsidered.
“Importantly, vaccination:
• protects against infection;
• protects against adverse outcomes;
• reduces transmission of COVID.
“The booster dose will give further protection against COVID and once evidence on spread after the third dose has been assessed inclusion of more people could be warranted.”
Prof Peter Openshaw, Professor of Experimental Medicine, Imperial College London, said:
“If someone in your household has COVID-19, how likely are you to catch it?
“This is an interesting ‘real life’ study of household transmission in the UK performed by a brilliant collaboration between researchers from Imperial College London, the UK Health Security Agency (UKHSA, formerly PHE) and the Manchester Foundation NHS Trust.
“Our Health Protection Research Unit (HPRU in Respiratory Infections) investigated the factors that affect household transmission. They followed 621 people with mild to moderate COVID-19; some were ‘breakthrough’ infections in vaccinated people (14 Pfizer–BioNTech, 23 Oxford–AstraZeneca, 1 Sinovac). Infections in those who had been double-vaccinated cleared more quickly, but peak viral loads were similar. These similar peak viral loads in vaccine breakthrough infections may explain why infected vaccinated people were just as likely to pass on infection as infected unvaccinated people.
“So, what about the uninfected people in the household of those with infections? One quarter (25%, 31/126 contacts) of double-vaccinated household members became infected compared to 38% (15/40) of unvaccinated contacts. The protection against nasal infection was most evident during the first 3 months after the second dose.
“So you have a good chance of not getting infected if you are living with someone with COVID and your chances are better if you have been recently double-vaccinated. However, if you want to avoid being infected you still need to do everything you can to avoid close contact, wear a mask and wash your hands even if you have been vaccinated.”
Prof Paul Hunter, Professor in Medicine, UEA, said:
“This study is not the first to show transmission within households even between vaccinated individuals and before the appearance of the delta variant (for example see https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.31.2100640), nor is it the first to suggest that ill vaccinated people can shed similar levels of virus as ill un vaccinated people (e.g. https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm?s_cid=mm7031e2_w).
“Nevertheless, this paper represents a clear analysis of the dynamics of the virus in vaccinated cases and their vaccinated and non-vaccinated contacts and as such is a valuable contribution. This study took place between September 2020 and September 2021 and included index cases with pre-alpha, alpha and delta variant infections but transmission analyses were restricted to delta index cases and so estimates of transmission risk are still probably current.
“The main observations to my mind are:
“1. That viral peak viral is similar in vaccinated and unvaccinated cases, though viral load declines somewhat more rapidly in vaccinated individuals. This finding is not surprising but could be subject to misunderstanding. What we do know is that vaccinated people are rather less likely to get sick from COVID compared to unvaccinated people. But when they do get sick the severity of illness is broadly corelated with viral load https://www.nature.com/articles/s41467-020-19057-5 and so it is not surprising that similarly ill people will shed roughly the same amount of virus whether vaccinated or not. So this finding does not mean that vaccinations are not doing an effective job and this can be seen in the secondary attack rates in household contacts where the protective effect of full prior vaccination prior to exposure is clear. But Infection in this paper is through PCR tests of swabbing regardless of symptoms in contacts and as we know from other studies vaccines are better at preventing symptomatic (especially severe illness) than asymptomatic illness, so this paper cannot be used to indicate vaccine effectiveness against severe disease.
“2. This paper shows that although peak viral load is the same in both vaccinated and unvaccinated index cases, viral load declines somewhat more rapidly in vaccinated individuals. There is some evidence that this may reduce the risk to contacts but numbers are not sufficient to give very different secondary attack rates. This probably is because the period that cases are most infectious between 2 days before until 3 days after symptom onset which is the period of peak viral load https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2783099. Consequently, a more rapid decline in viral load would be expected not to have that much of an impact. But what the authors do show is that household transmission whatever the vaccination status of secondary contacts is more frequent than previously reported for other variants.”
Dr Simon Clarke, Associate Professor in Cellular Microbiology, University of Reading, said:
“These findings show that the vaccines remain an effective way to drive down Covid-19 infection, but they are not a silver bullet. Infection in the wider community can still be amplified by transmission at home.
“The paper confirms a lot of what was either already known or suspected and it reports a well conducted and useful study. Most transmission of the delta variant occurs in the home, but it would be a grave mistake to assume that households are the only place where it occurs, someone has to take it into the home by picking it up somewhere else. Similarly, people will take it out of the home and without transmission in the wider community, Covid-19 would have run out of steam a long time ago.
“Home transmission was found to be quite high in fully vaccinated households, but higher still in unvaccinated ones. The vaccines reduce viral transmission, but don’t completely stop it.
“Vaccinated individuals who become infected can be effective transmitters of the virus and at their peak, have as much of it in their airways as someone who has not been vaccinated. However, they’re unlikely to transmit high quantities of virus for as long as someone who’s unvaccinated. This, coupled with the fact that a vaccine reduces someone’s chance of getting infected in the first place, means that while the vaccines don’t provide complete protection against transmission, they are not completely ineffective.”
Prof Rowland Kao, the Sir Timothy O’Shea Professor of Veterinary Epidemiology and Data Science, University of Edinburgh, said:
“The results of this study are consistent with what we already know about the delta variant, which, while vaccination is somewhat protective against infection (and highly protective against severe infection), delta remains very good at transmitting to people who have been vaccinated, or even double vaccinated.
“The estimates for high rates of transmission in household also highlights the roles that households play in spreading COVID – long term close contact indoors being perhaps the most important risk factor for transmission. Here, the interaction between community or schools-related transmission amongst younger adults and teens which may spread disease from household to household and household interactions with older and possibly more vulnerable individuals is particularly important. This interaction emphasises the need for the two-pronged approach of rapidly deploying vaccines to teenagers and boosters to vulnerable individuals; the vaccinations of younger persons to slow down transmission in the community, and the boosters to directly protect against severe infection and hospitalisation.
“Finally, the result that vaccinated individuals who become infected appear to pose a similar infection risk to others also emphasises the need for continued or improved non-pharmaceutical interventions to further slow down transmission rates and ease hospital burdens over the winter, having the added advantage that further risks due to other respiratory infections (flu and RSV being of primary concern) could also be mitigated by NPIs.”
Prof Penny Ward, Independent Pharmaceutical Physician, Visiting Professor in Pharmaceutical Medicine at King’s College London, said:
“It’s tough running household studies in respiratory illnesses, as I know from having run a couple investigating impact of treatment and/or chemoprophylaxis as a means to reducing household transmission.
“This is an elegant study from the ATACCC study group, demonstrating the science behind the observed ongoing delta variant fueled COVID outbreak – namely that fully vaccinated people unfortunate enough to develop COVID can transmit infection to others with whom they are in close contact at similar frequency (25%) to an unvaccinated case (23%).
“Participants in this study provided daily nasopharyngeal swabs enabling the study team to evaluate the impact of vaccination on peak viral load (almost none) and viral clearance (slightly faster) demonstrating that vaccination is primarily a means of preventing serious complications of infection within an affected individual, rather than a means to control spread of infection within communities.
“One additional finding suggested by the timing of symptomatic infection relative to vaccination is that waning individual protection may occur from 3 months rather than the 6 months currently scheduled for booster doses.
“The authors suggest other non pharmaceutical interventions are required to reduce infections and prevent onwards household transmission. The former is difficult to achieve without dealing the economy another hit and the latter is very difficult, particularly in smaller houses with high occupancy rates as is often the case in the UK. Perhaps the authors could continue their studies by investigating the use of pharmaceutical interventions – be these monoclonal antibodies or oral medicines – to treat the cases and offer post exposure prophylaxis to the rest of the household. I’m willing to bet that transmission would be smartly curtailed using these. Here’s an example of such a study design: Hayden, Frederick G., et al. “Management of Influenza in Households: A Prospective, Randomized Comparison of Oseltamivir Treatment with or without Postexposure Prophylaxis.” The Journal of Infectious Diseases, vol. 189, no. 3, Oxford University Press, 2004, pp. 440–49, http://www.jstor.org/stable/30076977. Let’s use the emerging pharmaceuticals coming on line to get this epidemic under proper control.”
‘Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study’ by Anika Singanayagam et al. was published in The Lancet Infectious Diseases at 17:00 UK time on Thursday 28 October 2021.
DOI: 10.1016/S1473-3099(21)00648-4
Declared interests
Prof Peter Openshaw: “Peter Openshaw has served on scientific advisory boards for Janssen/J&J, Oxford Immunotech, GSK, Nestle and Pfizer in relation to immunity to viruses (fees paid to Imperial College London).”
Prof Penny Ward: “I am semi-retired, but I am owner/Director of PWG Consulting (Biopharma) Ltd a consulting firm advising companies on drug and device development. Between December 2016 and July 2019 I served as Chief Medical Officer of Virion Biotherapeutics Ltd, a company developing antiviral treatments for respiratory viral diseases. Previous employee of Roche, makers of tocilizumab (anti IL6 antibody) and CMO of Novimmune, makers of empalumab (anti IFN gamma antibody).”
None others received.